

Introduction:
SARS-CoV-2 coronavirus (COVID-19) associated coagulopathy leads to higher morbidity and mortality. It is unclear if anticoagulants or antiplatelets in patients with COVID-19 influences disease severity. We report outcomes of COVID-19 patients prescribed anticoagulants or antiplatelets for preexisting conditions within Kaiser Permanente Northern California (KPNC), a large integrated health system serving 4.4 million members.
Methods:
This retrospective cohort study included KPNC adult members (≥18 years) with positive COVID-19 testing between February 25,2020, and May 8,2020. Patients were stratified based on electronic medical records indicating a filled prescription or actively taking antiplatelets or anticoagulants within 90 days prior to COVID-19 diagnosis.
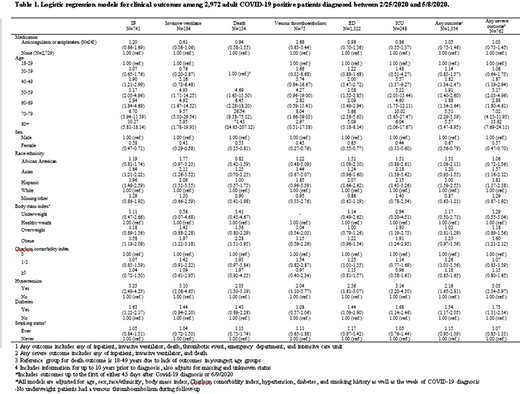
Primary outcomes included emergency department (ED) visit, inpatient hospitalization, intensive care unit (ICU) stay, venous thromboembolism (VTE), mechanical ventilation, and mortality between date of COVID-19 diagnosis and the first of either 45 days after diagnosis or 6/9/2020. Any severe outcome was defined as any of inpatient hospitalization, mechanical ventilation, or mortality. Logistic regression was used to calculate odds ratios and 95% confidence intervals (CI) for the association of anticoagulants or antiplatelets with primary outcomes, adjusting for sociodemographic and clinical characteristics. Models were adjusted for week of diagnosis given changing testing and treatment guidelines over time.
The Research Determination Committee for KPNC has determined the project does not meet the regulatory definition of research involving human subjects per 45 CFR 46.102(d).
Results:
Of 2,972 patients with confirmed positive COVID-19, 167(6%) were on antiplatelets, 69(2%) were on anticoagulants, and 7(<1%) on both. Most patients on anticoagulants or antiplatelets were older (77% aged >60 years), non-white (53%), overweight or obese (69%), and had >3 comorbidities (62%).
After adjusting for sociodemographic and clinical characteristics, chronic anticoagulants or antiplatelets use was not associated with a lower risk of any primary outcome, including VTE, ED visit, ICU stay or severe outcome (OR 1.03, CI 0.74-1.45). Older patients had an increased risk of all outcomes except VTE, with the highest risk of severe outcomes in those > 80 years compared to 18-29 years (OR 13.62, CI 7.69-24.11). Male patients and Asian or Hispanic patients (compared to white patients) also had increased risk of severe outcomes. A higher mortality risk was noted in patients with underlying obesity (OR 2.28, CI 1.31-3.95) and hypertension (OR 2.03, CI 1.30-3.19), but not with diabetes (OR 1.43, CI 0.89-2.28). (Table 1)
Conclusions:
This analysis using a socio-demographically diverse cohort of COVID-19 positive patients demonstrated that patients on chronic anticoagulants or antiplatelets did not have lower risk for inpatient hospitalization, invasive ventilator, or death. There was a significantly higher risk of severe outcomes in those with older age, Asian or Hispanic ethnicity, male gender, obesity, hypertension and diabetes.
Infection with COVID-19 can lead to a severe systemic inflammatory response, vascular endothelial dysfunction and hemostatic derangements, predisposing to microvascular and macrovascular thrombi and significant morbidity. Efforts to mitigate the disease severity have generated discussions regarding empiric use of anticoagulants and antiplatelets in COVID-19 patients. We did not find a difference in the risk of hospitalizations, mechanical ventilation or death for patients on chronic anticoagulants or antiplatelets. Our findings argue against the empiric use of these agents at COVID-19 diagnosis until prospective studies powered to evaluate thrombosis risk and clinical outcomes with value to patients and health care systems are completed.
The major strength of this study included the availability of all outcomes data for inpatients and outpatients with COVID19. Limitations include possible missed data from undiagnosed COVID-19 patients due to evolving COVID-19 testing and variance in inpatient treatments which may influence outcomes. Despite this, our findings do not suggest a clinical benefit of chronic anticoagulants or antiplatelets in mitigating disease severity in COVID-19 patients
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal